소아 비만과 소아 비만증, Obese and obesity in children 1/30/2022
소아 비만증의 역학
- 소아 비만과 소아 비만증은 어느 나라나 어느 지역에 국한되어 발생되는 것이 아니라 전 세계적으로 발생되고 발생률이 증가 추세에 있다.
- 미 사춘기 전 아이들과 사춘기 아이들 중 16.3%가(2003~2006년) 비만증에 걸려있다고 한다(출처; Contemporary pediatrics, December 2008. p.505). 다행히도 최근 비만증 발생률이 감소 추세에 있다(미국 CDC 2012년도 보고)
- 또 소아 비만증은 비만증이 있는 아이 본인은 물론이고 그의 가정과 국가 전반에 걸쳐 경제, 건강, 교육, 사회, 정신, 육체적 면에서 부정적으로 영향을 미친다.
비만과 비만증의 정의
- 신체 질량 지수(체격지수/BMI/Body-mass lndex)의 수치에 따라 소아 비만을 정의한다.
-
- 어떤 아이의 신체 질량지수가 그 아이의 나이, 성별, 인종과 같은 또래들의 신체 질량지수의 95백분율과 동등하거나 그 이상 더 높으면 그 아이는 비만하다고 정의할 수 있고, 그 비만으로 생긴 증상을 비만증이라 한다.
- 신체 질량 지수의 백분율이 85~94 백분율에 속하는 아이들을 과 체중아들이라고 하고, 과 체중아들의 대부분은 앞으로 계속 비만해 질 수 있는 가능성이 아주 높다.
- 아이의 체중(단위는 kg)과 신장(단위는 meter)을 재고 그 신장 치를 자승해서 나온 수치로 체중 치를 나누어 나온 수치를 신체 질량 지수(BMI)라고 한다.
- 즉, 체중(kg)/(신장 (m))X(신장 m)=신체 질량 지수(BMI)이다.
- 아이들의 체중 치를 X선으로 정하고 신장 치를 Y선으로 정한 후 각 체중 치와 신장 치가 만나는 XY점을 연결해서 만든 차트를 신체 질량 지수 차트(BMI chart)라고 한다.
- 어떤 아이의 체중 치와 신장 치가 얼마인지 알면 그 아이의 신체 질량 지수를 계산할 수 있고 그 지수를 신체 질량 지수 차트에서 어디에 있나 찾아 볼 수 있다.
- 신체의 수분의 총량과 신체의 지방의 총량의 비율을 계산해서 소아 비만을 진단 할 수 있다.
- 신체의 총 칼륨(K) 양으로 비만을 진단할 수 있고 TOBEC으로 비만을 진단할 수 있다. 이 방법으로 소아 비만을 정의하는 것은 임상적 실용 가치가 없어서 이 방법으로 소아 비만을 진단하는 경우는 드물다.
- 지방이 피하 조직을 비롯해 신체의 다른 부위에 많이 축적되어 전신이 비정상적으로 뚱뚱하게 보이면 비만하다고 정의한다.
- 어떤 아이의 체중이 그 아이의 나이, 성별, 인종, 신장과 같은 또래들의 체중보다 20% 이상 더 무거우면 비만하다고 정의 한다.
- 비만 진단용 의료기구로 잰 피하 지방층의 두께가 정상보다 더 두꺼울 때 비만하다고 진단할 수 있다.
- 체중과 신장을 재고 몸집을 육안으로 보고 비만한 것 같이 보이면 비만하다고 진단하는 것이 일반적이다.
- 어떤 아이의 피하 지방층의 두께가 동년배들의 피하 지방층 두께보다 더 두껍지는 않지만 골격과 근육이 더 잘 발달돼서 동년배들보다 체중이 더 나갈 수 있다. 이 경우 그 아이가 비만하다고 진단지 않는다..
- 다시 설명하면, 어떤 아이의 체중이 동년배들의 체중보다 좀 더 무겁거나, 동년배들보다 골격과 근육이 더 발달돼서 비만한 것 같이 보이지만 피하 지방층이 현저하게 두껍지 않으면 비만하다고 진단할 수 없다.
- 어떤 아이의 근육과 골격이 동년배들의 것보다 정상적으로 훨씬 더 크고 잘 발달되어 체중과 신장이 동년배들의 것보다 훨씬 더 나갈 때 그 아이는 동년배들보다 더 크다고는 할 수 있지만 비만하다고 진단할 수 없다.
- 이런 저런 이유로 비만을 정의하는 것이 때로는 상당히 복잡하다.

Copyright ⓒ 2012 John Sangwon Lee, MD.,FAAP
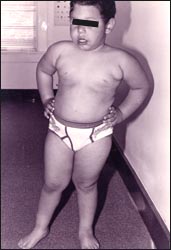
사진 1-79.체중이 40Kg 인 큰 4세 남 유아. 골격과 근육이 잘 발육됐지만 신체 질량 지수에 의하면 비만하지 않다.
Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
비만의 기전
- 비만해지는 기전(비만 기전)은 복잡하다.
- 그러나 비만해지는 기전을 잘 이해하면 비만과 비만증을 진단 치료 예방하는데 많은 도움이 된다.
- 비만해지는 기전을 구체적으로 살펴보면,
- 섭취한 음식물의 대부분은 위장관 속에서 포도당, 지방산, 아미노산 등으로 소화된 후 위장관 점막층을 통과 한 후 핏속으로 흡수된다.
- 그날그날 섭취한 음식물에서 얻은 영양분과 에너지(칼로리) 중 일부는 그날그날 평소 활동 하고 인간 기본 생명 유지를 하는데 에너지 자원으로 사용되고 일부는 그날그날 계속 성장 발육하는 자원으로 쓰인다.
- 나머지 영양분과 칼로리는 앞으로 그때그때 평소 활동 하고 인간 기본 생명 유지를 하는데 필요할 때마다 쓸 수 있게 간과 근육 등에 당원(글리코겐)으로, 또는 피하 지방 조직층 등에 지방질로 저장된다. 그렇게 저장된 당원과 지방은 일상생활을 할 때 필요에 따라 쓸 수 있는 에너지 자원이 된다.
- 나이에 따른 성장 발육에 필요로 하는 영양분과 평소 활동하는데 필요로 하는 영양분과 에너지의 양보다 더 많은 영양분의 양과 에너지의 양을 그 날 섭취할 때 그 날 성장 발육하고 평소 활동을 하는데 쓰고 남은 영양분의 양과 에너지의 양은 근육과 간 등에 당원으로 저장되고 지방질로 저장된다.
- 이 때 성장 발육하고 평소 활동하는데 필요로 하는 이상 더 많이 섭취했던 영양분의 양과 에너지 양을 지방질로 축적된다.
- 피하 지방 조직이 더 두꺼워지고 지방 조직에 소위, 살이 찌게 되고 그로 인해서 비만해질 수 있다.
- 그와 반대로, 그날그날 성장 발육하고 평소 활동하는데 필요로 하는 영양분과 에너지의 양보다 더 적은 영양분과 에너지를 섭취할 때는 근육과 간 등에 당원으로 저축되지 않고 지방질이 더 이상 저축되지 않는다.
- 이 경우, 근육과 간 등에 저축되었던 당원과 피하 지방 조직에 저축됐던 지방질을 그때그때 필요에 따라 에너지 자원으로 쓰게 된다.
- 그래서 지방질이 축적되기보다 지방질이 빠지고 몸이 빼빼해진다.
- 나이, 성별, 인종, 체중이 같은 두 아이가 같은 종류, 같은 양의 음식물을 섭취한 후 그 중 한 아이는 다른 아이보다 육체적 운동을 더 많이 해서 그 날 섭취한 음식물에서 나온 에너지와 영양분의 양보다 더 많은 에너지와 영양분의 양을 소모하면 지방질이 축적되지 않고 이미 축적되었던 지방질이 빠질 것이다.
- 그와 반대로 다른 아이는 먼저 아이보다 육체적 운동을 덜 하고 평소에 주로 앉아있거나 TV를 많이 보고 앉아서 컴퓨터 게임 등으로 대부분의 시간을 소일하면 그 날 섭취한 음식물로 얻은 에너지의 양보다 더 적은 에너지의 양을 소비하게 된다.
- 그 아이가 그날그날 성장 발육하는 데 쓰고, 활동하는데 쓰고 남은 에너지와 영양분의 양은 간이나 근육 등에 당원으로 저축되고 피하 지방 조직이나 다른 신체부위에 지방질로 저장되어 살이 찌게 될 것이고 비만해질 수 있다.
- 이상 설명한 바와 같이 어떤 아이가 자기 동년배들보다 음식물을 더 많이 먹는다고 해서 꼭 더 비만해지는 것이 아니다.
- 자기 동년배들보다 음식물을 더 적게 먹은 후 평소 육체적 운동을 적게 하면 그날 얻은 칼로리 양이 덜 소비되고 비만해질 수 있다.
소아 비만과 비만증의 추정 체중 퍼센타일
- 8~15세의 남아들이나 여아들의 체중 백분위선이 50 퍼센타일(Percentile)이면 그 아이들이 성인이 될 때의 체중이 과체중 성인들이 될 가능성이 많다.
- 8-15세의 여아들이나 남아들의 체중 백분위선이 50-75 퍼센타일이면 체중 백분위선이 50퍼센타일 이하에 속하는 아이들에 비해 5배 정도 과체중아가 될 가능이 있고,
- 8-15세의 남아들이나 여아들의 체중 백분위선이 75-84 퍼센타일이면, 체중 백분위선이 50퍼센타일 이하에 속하는 아이들에 비해 20배 정도 과체중아가 될 가능이 있다고 한다. 참초문헌-7
- 1~3세의 유아들의 체중은 그 아의가 장차 비만아가 될 수 있느냐, 또는 될 수 없느냐를 결정질 수 있는 중요한 체중이라고 한다.
- 연구에 의하면, 4%의 1세 유아들의 체중이 초과 중량이었고
- 8%의 유아들이 비만했고
- 16%의 3세 유아들의 체중이 초과 중량이었고,
- 30%의 유아들이 비만 했다고 한다(출처-Pediatric News, July 2007).
소아 비만과 비만증의 합병증
- 과체중, 비만, 비만증이 성인들에게도 많이 생기고 소아청소년들에게 많이 생기는 추세에 있다. 또 그로 인해 각 개인은 물론이고 국가적 차원에서 볼 때 나라의 범국민 건강 문제로 등장하고 있다.
- 미 2~5세 유아들의 26%가 비만하거나, 비만에 가깝다고 한다.
- 사춘기가 되기 전에 생긴 소아 비만은 사춘기가 된 후 사춘기 비만으로 이어지고, 사춘기의 비만은 성인기 비만으로 이어진다.
- 과체중이나 비만 또는 비만증이 있는 아이들이나 성인들에게 과유지질증, 고혈압, 천식, 2형 당뇨병 등의 발생률이 높다.
- 그 합병으로 사망률이 비만하지 않은 성인들에게 훨씬 더 높다(출처; Archives of Pediatrics & Adolescent Medicine. April 2008.
소아 비만과 비만증의 원인
- 친 부모 형제자매들 중 누군가가 타고날 때부터 뚱뚱한 체질이고 비만하면 친 부모 형제자매들도 뚱뚱한 체질을 가질 수 있고 비만할 수 있다. 대부분의 비만은 유전성이 있다.
- 빈곤한 가정에서 사는 아이들 중 일부에게 더 비만할 수 있다.
- 모유나 인공영양만 먹어야 할 영아들에게 너무 이른 나이에 이유식을 많이 먹인다든지 너무 많이 먹이면 쉽게 비만해진다.
- 중추신경계 질환, 내분비선계 질환, 또는 정신 이상 등으로 비만해 질 수 있다.
- 배가 고프지도 않은데 부모의 조건 없는 진정한 사랑이 필요해서 울고 보챌 때 조건 없는 진정한 사랑을 해 주는 대신 인공영양 및, 또는 이유식 등을 부모의 사랑대신 자주 많이 먹이면 비만해 질 수 있다.
- 평소에 먹은 음식물에서 얻는 칼로리의 양보다 육체적 활동으로 소모된 칼로리의 양이 적으면 비만해 질 수 있다.
- 근육이 발달되고 체격이 크거나 뚱뚱하고 큰 체격이 건강상 더 좋다고 믿는 부모들은 자녀들에게 음식물을 필요 이상으로 더 많이 주어 비만해 질 수 있다.
- 삶의 질이 낮게 사는 가족들에게 비만이 더 쉽게 생길 수 있고 심지어는 수면부족도 생길 수 있다(출처; Pediatric News, September 2008).
- 렘(REM) 수면 기간이 짧으면 비만해 질 수 있다(출처; Pediatric News, September 2008, p.45).
- 갑상선 기능 저하증이 있으면 비만해 질 수 있다.(출처; Pediatric News, June 2008, p.34).
- 우울증이 있으면 비만해 질 수 있다.
- 1일 총 수면 시간이 12시간 이하로 자는 영아들은 비만 되기 쉽다(출처; Archives of Pediatrics & Adolescent Medicine. April 2008).
- 그 외
소아 비만과 비만증의 증상 징후
- 비만으로 생기는 증상을 비만증이라 한다.
- 비만의 정도에 따라 증상 징후가 다르다.
- 비만증이 있는 아이들을 관찰해 보면 비만증의 증상 징후를 쉽게 알 수 있다.
- 비만증의 전형적인 증상 징후를 구체적으로 설명한다.
- 비만증이 있는 아이들의 키는 동년배들의 키보다 좀 더 크고,
- 체중이 더 무겁고,
- 코와 입이 더 작게 보인다.
- 턱 주름살이 횡으로 잡혀 있는 것이 보통이다.
- 비만증이 있는 남아들의 유방은 성인 여성 유방 형과 같게 클 수 있지만
- 비만한 아이들의 젖꼭지는 성인 여성 형 젖꼭지 같이 크지 않고 발육되지 않고 유륜도 발육되지 않는다.
- 앉아 있을 때 주름살이 뱃가죽에 가로로 크게 잡혀 있고,
- 자지의 대부분이 음부 살갗 속으로 묻혀 있기 때문에 자지가 비정상적으로 작아 보이는 것이 보통이다.
- 비만증이 있는 사춘기 아이들의 2차 성징 발육은 비만증이 없는 동년배 사춘기 아이들보다 좀 더 일찍 오는 것이 보통이다.
- 상지는 비교적 더 짧은 편이고 하지는 비교적 더 길고,
- 육체적 운동을 활발하게 하기 어렵고 일상생활을 할 때 동작이 좀 느린 편이다.
- 비만증이 있는 아이들의 골격의 크기는 비만증이 없는 또래들의 골격의 크기와 거의 비슷하지만 체중은 동년배들의 것보다 더 무거운 것이 보통이다.
- 넓이 뛰기, 달리기, 또는 다른 종류의 육체적 운동을 할 때 체중이 더 무겁기 때문에 동년배들보다 더 잘 할 수 없다.
- 비만으로 신체 상이 이상하기 때문에 학교에서나, 집에서 또는 남들 앞에서 겉옷이나 속옷을 벗어야 할 때도 옷을 벗는 것을 싫어하고
- 단체 운동에 참가하기를 싫어하는 것이 보통이다.
- 서 있을 수 있고 앉아 있을 수 있는 상황에서 서 있기보다 앉아 있는 것을 선택하는 것이 일반적이다.
- 비만증이 있는 아이들에게 비만으로 불리한 점이 더 많이 있고 고민도 많고 걱정을 많이 하는 것이 보통이다.
- 비만한 아이들이나 성인들은 어디서든지 언제든지 음식물을 먹기를 좋아한다.
- 아주 심한 비만증을 가지고 있는 아이들에게 호흡곤란, 고혈압, 2형 당뇨병, 고관절 탈구 등의 건강 문제가 더 쉽게 생길 수 있고
- 비만 수술치료를 받을 때는 회복할 때도 불리한 점이 많다.
- 일반적으로 비만증을 가진 성인들의 평균 수명은 비만증이 없는 성인들에 비해 더 짧은 편이다.

사진 1-80.비만증이 있는 3세 남아의 유방
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP

사진 1-81. 배에 생긴 신장반(스트레치 마크)
Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
비만과 공존 이환
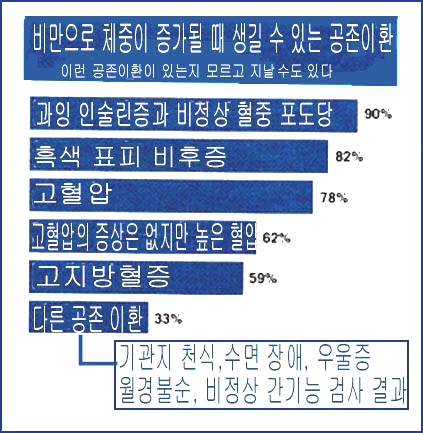
그림 1-85. 비만과 공존 이환
출처-Dr. Auron-Gomez and Elsevier Global Medical News
Pediatric News, July 2007
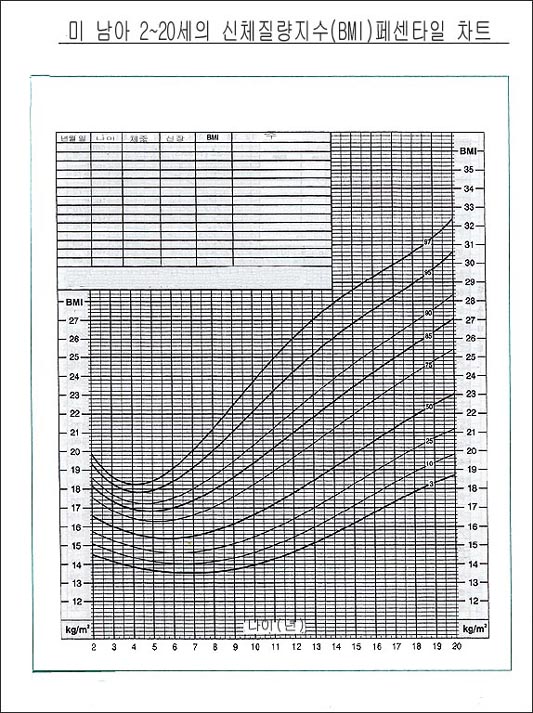
그림 1-82.2-18세 남아들의 신체 질량 지수수(Body-mass lndex, BMI) 퍼센타일 차트
출처 – CDC, USA
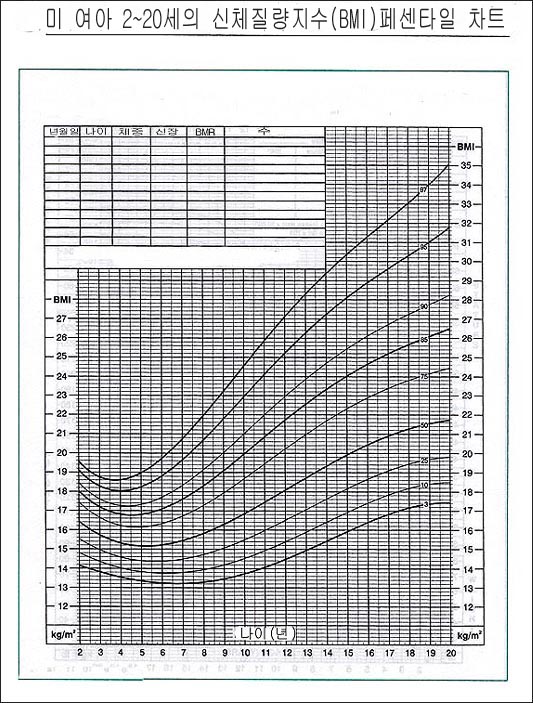
그림 1-83. 2-20세 여아들의 신체 질량 지수 퍼센타일 차트
출처 – CDC, USA
소아 비만, 소아 비만증, 과체중의 진단
- 병력, 증상 징후, 진찰소견 등을 종합해 소아 비만, 소아 비만증, 소아과 체중을 진단할 수 있다.
- 소아 정기 건강검진을 받을 때 마다 체중, 신장을 재고 신체 질량 지수 차트(BMI chart)에서 각 아이의 신체 질량 지수 수치를 찾아 비만한지 비만증이 있는지 과체중인지 진단받을 수 있다.
- 모든 소아청소년들이 소아 건강검진을 받을 때마다 신체 질량 지수가 얼마인지 반드시 알아야한다.
- 건강검진을 받을 때 혈압, 호흡 수, 맥박 수, 체온 등 바이탈 사인(생명 징후)을 알아보는 것 같이 신체 질량 지수 수치를 통상적으로 알아보는 것이 중요하다.
- 소아청소년의 신체 질량 지수 수치가 95퍼센타일 이거나 그 보다 더 높은 퍼센타일이면 비만하고, 또는 30kg/㎥이상 되면 비만하다고 할 수 있다.
- 만일 소아 신체 질량 지수 수치가 85퍼센타일 이거나 그 보다 더 높거나 신체 질량 지수의 수치가 95퍼센타일 이하면 그 소아는 과체중 아에 속한다.
- 피하 지방 조직 두께를 특수 의료 기구로 측정해 비만을 진단할 수 있으나 요즘 진단 방법으로 진단하지 않는다(p.00 비만의 정의 참조).
표 1-16.소아기 비만증에 관련된 병원 입원 환아들의 병명
| 진단 병명 | 병원 입원 수 |
| 당뇨병 | 9,503 |
| 임신과 그에 관련된 병 | 18,086 |
| 감정 질환 | 29.074 |
| 천식 | 16,251 |
| 골격 질환 | 4,319 |
| 충수염 | 7,801 |
| 폐렴 | 5,679 |
| 담도질환 | 5,663 |
| 전신질환 | 7,455 |
| 피부와 피하조직 감염 | 5,914 |
| 정신 분열증 | 4,808 |
출처와 참조문헌:Trasande L Health Aff.2009: 28: 751-760
소아 비만과 비만증의 치료
- 비만의 원인은 단순하지 않고 복잡하기 때문에 치료가 쉽지 않고 복잡하다.
- 학동기 이전 아이들의 비만을 치료 하는 것이 중요 하다 (소스:Pediatrics 8/2019).
- 계속 성장 발육하는 있는 소아청소년들이 인간 기본 생명 유지에 그날그날 필요로 하는 칼로리 양과 영양분의 양과 그날그날 하는 육체적, 정신적 운동량이 얼마인지 정확하게 알기 어렵다.
- 때문에 그날그날 섭취한 음식물에서 얻는 영양분과 칼로리의 양과 평소 생활을 할 때의 소모되는 총 에너지(칼로리)와 영양분의 양을 조절해서 비만증을 치료하기가 어렵다.
- 또한 아이들은 계속 성장 발육하기 위해 나이에 따라 균형 잡힌 음식물을 충분히 먹어야 하고 그와 동시에 체중과 신장도 매일 계속 성장해야 한다.
- 또 아이에 따라 매일매일 체중의 증가 속도가 다르다. 이런 여러 가지 복잡한 이유로 소아 비만은 음식물 섭취 양과 육체적 운동 양 등을 일률적으로 정해 놓고 그 근거에 토대를 두고 소아 비만을 치료하기가 어렵다.
- 그 때문에 소아가 비만해지기 전에 미리부터 비만을 예방하는 것이 이상적인 소아 비만 치료라고 할 수 있다.
- 소아 정기 건강검진을 하기 위해 소아청소년과로 자녀를 데리고 가서 체중과 신장을 재고 체중 질량 지수가 얼마 인가 알아보고 비만한지 알아보고 비만하면 치료를 시작하고 비만하지 않게 예방해야 한다.
- 비만한 아이들도 비만하지 않은 아이들과 똑같이 하루 주식을 세 번 꼭 먹어야 하고 필요에 따라 간식과 비타민도 먹어야 한다.
- 그렇지만 칼로리의 양이 더 많이 나가는 케이크 등 고 칼로리 음식물은 가능한 덜 먹어야 한다.
- 비만한 아이들이 그날그날 필요로 하는 칼로리 양을 나이와 체중에 따라 계산하고 그에 해당하는 음식물을 먹어서 비만을 치료하는 방법이 있지만 이 방법으로 치료가 잘 되지 않는 것이 보통이다.
- 심한 비만증은 소아청소년과 전문의, 소아 정신과 전문의, 소아 영양사, 부모와 그 아이 모두가 비만 치료 팀의 멤버가 되어 서로 합심해서 적극적으로 치료해야 한다.
- 아이의 체중, 나이, 그날그날 육체적 활동량의 정도에 따라 하루 동안 필요로 하는 칼로리 양을 계산해서 그에 해당되는 균형 잡힌 음식물을 먹고 심리요법, 적당한 육체적 운동으로 치료할 때도 있다.
- 일반적으로 소아 비만증은 약물로 치료하지 않는다.
- 그 외 비만증을 수술로도 치료 한다.
- 연구에 의하면, 저 탄수화 물질류 음식물 섭취가 저 지방질류 음식물류 섭취하는 것이 체중 조절 효과가 더 난다고 한다.소스;AMA Morning Rounds Wednesday, June 27, 2012
- 성인 비만 치료용 Lorcaserin이 미 FDA의 허가를 최근 받았다. Lorcaserin으로 BMI이 30 이상되는 성인 비만증 또는 2형 당뇨병, 이상 지질혈증 또는 고혈압이 있고 BMI이 27이상 되는 성인 비만증을 적절한 육체적 운동, 음식물 섭취 조절과 더불어 치료 할 수 있다.
- 아직 18세 이하 소아 비만증 치료에 쓸 수 있게 인가되지 안했다. Physician’s First Watch for June 28, 2012
비만 장기 치료제(성인)
|
Orlistat (Xenical) |
췌장 리파제 억제제로서 장관 지방 흡수 억제로 체중 감소 |
|
Lorcaserin (Belviq) |
세로토닌 2C 수용체 작용제로 장기 비만 체중 감소 치료 |
|
Sibutramine (Reductil or Meridia) |
식욕 억제제 또는 식욕 부진제 |
|
Rimonabant (Acomplia) |
식욕 부진제 |
|
Phentermine/topiramate |
약리 작용 잘 모름 |
|
buproprion-naltraxone |
항 우울증 약 |
|
Liraglutide(Victoza) |
글루카곤 비슷 펲타이드 (GLP) 1 수용체 자용제로서 뇌 식욕 조절 |
참조 및 소스:HARVARD MEDICAL SCHOOL, Endocrine CONTROVERSIES IN ADULT PRIMARY CARE PRACTICE MAY15~16 2015
Nelson Pediatrics Textbook 19th Ed.
표 5-2.나이, 신장, 체중에 따른 비타민, 단백질, 미네랄(무기질), 칼로리의 1일 필요량
Daily requirement of vitamins, proteins, minerals by ages
|
|
나이 (세) |
체중(kg) |
신장(cm) |
칼로리(kcal) |
단백질(gm) |
칼슘(gm) |
철(mg) |
비타민A I.U |
지이민 B1 (mg) |
리보플라빈 B2 (mg) |
니아신 B3 (mg) |
비티민 C (mg)
|
비타민 D (mg) |
|
남여 영유아 |
0~1/2 |
7 |
63 |
115/kg |
2.0/kg |
0.6 |
1.0/kg |
1,500 |
0.4 |
0.4 |
6 |
35 |
400 |
|
1/2~1 |
9 |
72 |
100/kg |
1.8/kg |
0.6 |
15 |
1,500 |
0.5 |
0.6 |
8 |
35 |
400 |
|
|
남여1~9세 |
1~3 |
13 |
87 |
1,200/1 일 |
25/1 일 |
0.8 |
15 |
2,00 |
0.6 |
0.8 |
8 |
40 |
400 |
|
3~6 |
18 |
107 |
1,500/1 일 |
30/1 일 |
0.8 |
10 |
2,500 |
0.8 |
0.8 |
11 |
40 |
400 |
|
|
6~9 |
26 |
126 |
2,100/1 일 |
40/1 일 |
1.0 |
10 |
3,500 |
1.1 |
1.3 |
15 |
40 |
400 |
|
|
남9~18세 |
9~12 |
35 |
140 |
2,400/1 일 |
45/1 일 |
1.1 |
100 |
4,500 |
1.3 |
1.4 |
16 |
40 |
400 |
|
12~14 |
43 |
151 |
2,700/1 일 |
50/1 일 |
1.4 |
18 |
5,000 |
1.4 |
1.4 |
18 |
45 |
400 |
|
|
14~18 |
59 |
170 |
3,000/1 일 |
60/1 일 |
1.4 |
18 |
5.000 |
1.5 |
1.5 |
20 |
55 |
400 |
|
|
여 9~18세 |
9~12 |
35 |
140 |
2,200/1 일 |
50/1 일 |
1.1 |
18 |
4,5000 |
1.1 |
1.3 |
15 |
40 |
400 |
|
12~14 |
44 |
154 |
2,300/1 일 |
50/1 일 |
1.3 |
18 |
5,000 |
1.2 |
1.5 |
15 |
45 |
400 |
|
|
14~18 |
53 |
158 |
2,300/1 일 |
55/1 일 |
1.3 |
18 |
5,000 |
1.2 |
1.5 |
15 |
50 |
400 |
| 나이 (년) |
체중 (kg) |
신장 (cm) |
칼로리 (kcal) |
단백질 (g) |
칼슘 (g) |
철 (mg) |
비타민 A I.U. |
지아민 B1 (mg) |
리보플 라빈B2 (mg) |
니아 신 B3 (mg) |
비타 민 C (mg) |
비타 민 D (I.U.) |
|
| 영아 | 0~1/2 1/2~1 |
7 9 |
63 72 |
kgx115 kgx100 |
kgx2.0 1.8 |
0.5 0.6 |
kgx1.0 15 |
1,500 1,500 |
0.4 0.5 |
0.4 0.6 |
6 8 |
35 35 |
400 400 |
| 남여 1~9세 아이 |
1~3 3~6 6~9 |
13 18 26 |
87 107 126 |
1,200 1,500 2,100 |
25 30 40 |
0.8 0.8 1.0 |
15 10 10 |
2,000 2,500 3,500 |
0.6 0.8 1.1 |
0.8 0.8 1.3 |
8 11 15 |
40 40 40 |
400 400 400 |
| 9~18세 남아 |
9~12 12~14 14~18 |
35 43 59 |
140 151 170 |
2,400 2,700 3,000 |
45 50 60 |
1.1 1.4 1.4 |
10 18 18 |
4,500 5,000 5,000 |
1.3 1.4 1.5 |
1.4 1.4 1.5 |
16 18 20 |
40 45 55 |
400 400 400 |
| 9~18세 여아 |
9~12 12~14 14~18 |
35 44 53 |
140 154 158 |
2,200 2,300 2,300 |
50 50 55 |
1.1 1.3 1.3 |
18 18 18 |
4,500 5,000 5,000 |
1.1 1.2 1.2 |
1.3 1.5 1.5 |
15 15 15 |
40 45 50 |
400 400 400 |
소아 비만증 수술 치료
- 심하게 비만하면 그로 인해 고혈압, 위식도 역류, 무호흡증, 기관지 천식, 퇴행성 관절 질환, 당뇨병, 다발성 난소 낭종 등의 공존이환(p.113 참조)이 생길 수 있다.
- 여아들에게 비만증이 생겨 체중이 증가되면 사춘기와 퓨버티(Puberty)가 더 조기에 올 수 있다.
- 심지어는 9세 여아들에게 퓨버티가 올 수 있다.
- 이 나이에 퓨버티가 온 아이들에게 자녀 생산 능력이 있을 수 있다.
- 비만이 심하고 고혈압, 위식도 역류, 무호흡증, 기관지 천식, 퇴행성 관절 질환, 당뇨병, 또는 다발성 난소 낭종 등의 공존이환이 있는 소아들을 식이요법 비만치료, 운동 비만치료, 정신 정서 비만치료 등으로 적극적으로 치료해도 비만증이 적절히 치료 되지 않으면 심리 평가, 성장 발육 평가 등을 한 후 비만 루식 Y형 바이패스(Roux-en-Y gastric bypass) 수술치료로 비만증을 치료할 수 있다.
- 그러나 비만 수술치료로 치료하는 중 폐 혈전, 수술 부위 감염, 위 협착증, 위 소화성궤양, 또는 소장 폐쇄 등의 합병증이 생길 수 있다.
- 비만 수술치료로 12~19세 연령층 사춘기 아이들의 비만증을 치료할 수 있다고 한다.
- 요즘 미국 사춘기 아이들의 비만증을 복강경 위 밴딩(Laparoscopic gastric banding) 수술로 치료하기도 한다(그림 1-84 참조).
- 수술 받은 아이들의 비만증이 지속적 체중 감소로 치료된다고 한다. 수술치료에 의한 합병증은 성인들의 비만증 수술치료 때 생기는 정도와 비슷하다고 한다.
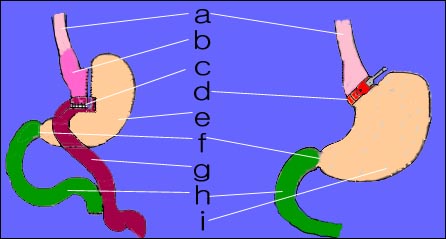
그림 1-84. 비만 루식 Y형 바이패스 수술치료
소아에 비만이 있고
- BMI가 95 퍼센타일이나 그 이상이고 다음 경우 중 한 가지 경우만 있으면 적절한 전문의의 자문을 얻도록 권장 한다.
-
- 당뇨병- 공복 혈당이 126mg/dl 이거나 그 이상에서부터 200mg/dl
- 장애 공복 혈당이125~120mg/dl
- 장애 공복 혈당 불래성 검사에서 140~199mg/dl
- 공복 인술인 혈당 농도가 25 이하
- 공복 LDL이 160 이상
- HDL이 40 이하
- triglycerides 300 이상
- 다낭 난소 증후군을 의심하거나
- 비 알코홀성 지방간을 의심 하거나
- BMI가 95 퍼센타일이거나 그 이상이고 다음 경우 중 2가지 이상 있으면 적절한 전문의의 자문을 얻도록 권장한다.
-
- 친 형제자매나 4촌 형제자매 중 2형 당뇨병, 고혈압, 조기 관상 동맥병, 남 55세 이전 뇌졸중이 있거나 여 65세 이전 뇌졸중이 있거나
- 흑색극소증
- 동양인, 흑인, 히스팬닉 등
소스:Connecticut Children’s Medical Center
|
다음은“소아 비만”에 관한 인터넷 소아청소년 건강상담 질의응답의 예 입니다. |
Q&A, 소아 비만
안녕하세요?
저는 이제 5살이 된 딸아이를 가진 엄마입니다.
애기 때부터 잘 먹고 잘 자는 습관이 있어서 그런지 지금껏 잔병치레 없이 잘 자라고 있는데요,
선생님께 여쭤보고 싶은 건 아동 나이별 체중과 키에 관해서 묻고 싶습니다.
저희 딸아이는 지금 3월이면 생일인 5세구요 키 105센티에 몸무게 19킬로입니다.
다른 아이에 비해 크고 좀 통통한 편이라 신경이 많이 쓰인답니다. 음식조절을 집에서 한다고 하는데 비만일 우려가 있을까요? 좀 걱정이 된답니다.
A.
안녕하세요.
좋은 질문을 해주셔서 감사합니다.
자녀의 나이, 성별, 과거 병력, 가족 병력, 진찰소견, 임상검사 등 자세한 정보가 더 많이 있을수록 더 좋은 답변을 드릴 수 있지만 주신 정보를 토대로 답변을 드리겠습니다.
체중은 75퍼센타일, 신장은 10퍼센타일 입니다.
조금 뚱뚱한 편이군요. 두 부모님도 아마 자녀와 같이 조금 뚱뚱할 것입니다.
비만을 참고하시고 아직도 문제가 계속 되거나 걱정이 되시면 소아청소년과에서 진찰 진단을 받으시고 그 문제에 관해 상담하시기 바랍니다.
질문이 더 있으시면 다시 연락 주시기 바랍니다. 감사합니다. 이상원 드림
.
Obese and obesity in children
Epidemiology of childhood obesity
• Childhood obesity and childhood obesity are not limited to any country or region, but occur worldwide and the incidence is increasing.
• It is reported that 16.3% of prepubertal and adolescent children in the US (2003-2006) are obese (source; Contemporary pediatrics, December 2008. p.505). Fortunately, the incidence of obesity has recently been on a downward trend (reported by CDC 2012 in the United States).
• Childhood obesity also negatively affects the economy, health, education, society, mental and physical aspects of children with obesity, their families, and the country as a whole.
Definition of Obese and Obesity
• Define childhood obesity according to the value of body mass index (Body index/BMI/Body-mass index).
• o If a child’s body mass index is equal to or higher than 95 percent of the body mass index of the child’s age, gender, and race, the child is defined as obese, and the symptoms resulting from the obesity are defined as obesity. it is said
o Children with body mass index percentages between 85 and 94 are called overweight children, and most overweight children are very likely to continue to be obese in the future.
o Measure the child’s weight (unit: kg) and height (unit: meter), and multiply the height by the square of the child’s weight.
o That is, body weight (kg)/(height (m))X(height m) = body mass index (BMI).
o The body mass index chart (BMI chart) is made by connecting the XY points where each weight value and height value meet after determining the children’s weight values on the X-ray and height values on the Y-line.
o Knowing what a child’s weight and height are, you can calculate the child’s body mass index and look up the index on a body mass index chart.
• Childhood obesity can be diagnosed by calculating the ratio of the total amount of body water to the total amount of body fat.
• Obesity can be diagnosed by the total amount of potassium (K) in the body, and obesity can be diagnosed by TOBEC. Defining childhood obesity with this method has no clinical practical value, so it is rare to diagnose childhood obesity with this method.
• Obesity is defined as excessive fat accumulation in the subcutaneous tissue and other parts of the body, making the whole body appear abnormally fat.
• A child is defined as obese if the child’s weight is 20% or more greater than the weight of the child’s age, gender, race, or height.
• Obesity can be diagnosed when the thickness of the subcutaneous fat layer measured with a medical device for diagnosis of obesity is thicker than normal.
• It is common to be diagnosed as obese when the weight and height are measured and the body looks obese.
• A child’s subcutaneous fat layer is not as thick as that of their peers, but their bones and muscles are more developed and they can weigh more than their peers. In this case, the child is not diagnosed as obese.
• In other words, if a child’s weight is slightly heavier than that of their peers, or they appear obese because their skeleton and muscles are more developed than their peers, but if the subcutaneous fat layer is not significantly thick, it cannot be diagnosed as obese.
• When a child’s muscles and skeleton are normally much larger and well-developed than those of their peers, and so weight and height are significantly higher than those of their peers, the child may be said to be larger than their peers but cannot be diagnosed as obese.
• Defining obesity for one reason or another is sometimes quite complex.
Picture 1-78. Obese 3-year-old boy. She weighs 35 kg. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
Picture 1-79. A large 4-year-old male infant weighing 40 kg. He has well-developed bones and muscles but is not obese according to his body mass index. Copyright ⓒ 2012 John Sangwon Lee, MD., FAAP
Mechanism of obesity
• The mechanism of becoming obese (obesity mechanism) is complex.
• However, a better understanding of the mechanism of obesity can help a lot in the diagnosis, treatment and prevention of obesity and obesity.
• If we look at the mechanism of obesity in detail,
• Most of the ingested food is digested into glucose, fatty acids, and amino acids in the gastrointestinal tract then passes through the gastrointestinal mucosa and is absorbed into the blood.
• Some of the nutrients and energy (calories) obtained from food eaten on a daily basis are used as energy resources for daily activities and basic human life support, and some are used as resources that continue to grow and develop day by day.
• The remaining nutrients and calories are stored as glycogen (glycogen) in the liver and muscles, or as fat in the subcutaneous adipose tissue layer, so that they can be used whenever necessary for daily activities and maintenance of basic human life. The stored sugar and fat become energy resources that can be used as needed in daily life.
• Nutrients that are needed for growth and development according to age and nutrients and energy that are more than the amount of nutrients and energy needed for normal activities The amount of energy and the amount of energy are stored as glycogen in muscles and liver, and as fat.
• At this time, the amount of nutrients and energy consumed more than needed for growth and development and normal activities is accumulated as fat.
• The subcutaneous adipose tissue becomes thicker and the adipose tissue becomes so-called fat, which can lead to obesity.
• Conversely, when you consume less nutrients and energy than you need for your daily growth and development and normal activities, your muscles and liver are not stored as sugar sources and fat is no longer stored.
• In this case, the glycogen stored in the muscles and liver and the fat stored in the subcutaneous adipose tissue are used as energy resources when needed.
• So instead of accumulating fat, fat is lost and the body is plump.
• After two children of the same age, sex, race, and weight eat the same type and amount of food, one of the children does more physical exercise than the other child, so the amount of energy and nutrients from the food eaten that day If you consume a greater amount of energy and nutrients, fat will not be accumulated and the fat that has already been accumulated will be lost.
• Conversely, if the other child does less physical exercise than the child and spends most of the time sitting mostly sitting or watching TV a lot, playing computer games, etc. amount is consumed.
• The amount of energy and nutrients that the child spends on daily growth and development, and the amount of energy and nutrients he spends on activities is stored as a sugar source in the liver or muscles, and stored as fat in the subcutaneous adipose tissue or other parts of the body, resulting in weight gain and obesity.
• As explained above, just because a child eats more food than their peers does not necessarily mean they will become obese.
• If you eat less food than your peers and do less physical exercise than your peers, you will burn fewer calories and become obese.
Estimated Weight Percentiles for Childhood Obesity and Obesity
• If the weight percentile for boys or girls aged 8-15 years is at the 50th percentile, they are more likely to be overweight adults when they reach adulthood.
• Girls or boys aged 8-15 years with a weight percentile of 50-75 percentile are five times more likely to be overweight than children with a weight percentile below the 50 percentile;
• Boys or girls aged 8-15 years with a weight percentile of 75-84 percentile are 20 times more likely to be overweight than children with a weight percentile below the 50 percentile. Chamcho Literature-7
• The weight of infants aged 1 to 3 is said to be an important weight that can determine whether or not the child can become obese in the future.
• Studies have shown that 4% of 1-year-old infants are overweight
• 8% of infants were obese
• 16% of 3-year-olds were overweight;
• 30% of infants are said to be obese (source-Pediatric News, July 2007).
Childhood obesity and its complications
• Overweight, obesity, and obesity are more common in adults and tend to occur more often in children and adolescents. As a result, it is emerging as a national health problem not only for each individual but also at the national level.
• 26% of children aged 2-5 years are obese or close to obese.
• Childhood obesity before puberty leads to puberty obesity after puberty, and puberty obesity leads to adult obesity.
• Children and adults who are overweight, obese or obese have a high incidence of hyperlipidemia, hypertension, asthma and type 2 diabetes.
• The mortality rate is much higher for non-obese adults (source; Archives of Pediatrics & Adolescent Medicine. April 2008.
Childhood obesity and causes of obesity
• If one of your biological parents’ siblings is born with a fat constitution and is obese, your biological parents’ siblings may also have a fat constitution and may be obese. Most obesity is hereditary.
• Some children from poor families may be more obese.
• Infants who need only breast milk or artificial nutrition will easily become obese if they feed too much or too much baby food at an early age.
• You may become obese due to central nervous system disease, endocrine system disease, or mental disorder.
• If you are not hungry, but you need true unconditional love from your parents, you can become obese if you frequently feed artificial nutrition or baby food instead of your parents’ love instead of giving true unconditional love when you cry.
• You can become obese if you burn fewer calories from physical activity than you get from the food you normally eat.
• Parents who are more muscular and of a larger body or who are obese and believe that a larger body is better for their health may become obese by giving their children more food than necessary.
• Families with lower quality of life may be more prone to obesity and even lack of sleep (source; Pediatric News, September 2008).
• Short periods of REM sleep can lead to obesity (source; Pediatric News, September 2008, p.45).
• Hypothyroidism can lead to obesity (source; Pediatric News, June 2008, p.34).
• Depression can make you obese.
• Infants who sleep less than 12 hours a day are more likely to become obese (Source; Archives of Pediatrics & Adolescent Medicine. April 2008).
• etc
Childhood Obesity and Symptoms, signs of Obesity
• Symptoms caused by obesity are called obesity.
• Symptoms vary depending on the degree of obesity.
• Observing children with obesity makes it easy to see the symptoms of obesity.
• Describe in detail the typical symptoms of obesity.
• Children with obesity are taller than their peers,
• You are heavier,
• The nose and mouth appear smaller.
• It is normal for the chin wrinkles to be held horizontally.
• The breasts of obese boys may be as large as that of an adult female, but
• The nipples of obese children are not as large and underdeveloped as the adult female nipples, and the areola is not developed.
• Wrinkles are large horizontally on the skin of the stomach when sitting,
• It is normal for the penis to look unusually small because most of it is buried in the skin of the genitals.
• Secondary sexual development in adolescents with obesity usually occurs earlier than in adolescents of the same age without obesity.
• The upper limbs are relatively short and the lower limbs are relatively longer;
• It is difficult to be active in physical exercise, and movements are a bit slow in daily life.
• The size of the skeletons of children with obesity are almost the same as those of their non-obese peers, but they are usually heavier than those of their peers.
• You can’t do better than your peers when you jump, run, or do other types of physical exercise because you weigh more.
• I hate taking off my clothes at school, at home, or in front of others because I have a strange body image because of my obesity.
• It is common to dislike participating in group sports.
• In situations where both standing and sitting are possible, it is common to choose to sit rather than stand.
• It is common for children with obesity to have more problems with obesity and to worry and worry a lot.
• Obese children and adults like to eat anywhere, anytime.
• Children who are very obese are more prone to health problems such as shortness of breath, high blood pressure, type 2 diabetes, and hip dislocations.
• There are many disadvantages when recovering from bariatric surgery.
• In general, the life expectancy of adults with obesity is shorter than those without obesity.
Picture 1-80. Breast of a 3-year-old boy with obesity Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Picture 1-81. Kidney plaques on the stomach (stretch marks) Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP Obesity and co-morbidities
Figure 1-85. Obesity and co-morbidities Source – Dr. Auron-Gomez and Elsevier Global Medical News Pediatric News, July 2007
Figure 1-82.2 – Body-mass index (BMI) percentile chart for boys aged 18 years Source – CDC, USA
Figure 1-83. Body Mass Index Percentile Chart for Girls 2-20 Years Old Source – CDC, USA
Diagnosis of childhood obesity, childhood obesity, and overweight
• It is possible to diagnose childhood obesity, childhood obesity, and pediatric overweight by synthesizing medical history, symptom signs, and examination findings.
• Every time children receive regular health check-ups, their weight and height are measured and each child’s body mass index value is found on the BMI chart to diagnose whether they are obese, obese, or overweight.
• It is essential that all children and adolescents know what their body mass index is at every pediatric health checkup.
• When undergoing a health checkup, it is important to routinely check your body mass index values, such as looking for vital signs such as blood pressure, respiration rate, pulse rate, and body temperature.
• Children and adolescents with a body mass index of 95 percent or higher are obese, or 30 kg/m or more are considered obese.
• If the child’s body mass index reading is at or above the 85th percentile, or the body mass index reading is below the 95th percentile, the child is considered overweight.
• Obesity can be diagnosed by measuring the thickness of the subcutaneous adipose tissue with a special medical instrument, but it is not diagnosed by modern diagnostic methods (see p.00 Definition of Obesity).
Table 1-16. Names of hospitalized children related to childhood obesity
표 1-16.소아기 비만증에 관련된 병원 입원 환아들의 병명
| 진단 병명 Diagnosis | 병원 입원 수 number of hospital admissions |
| 당뇨병 diabetes | 9,503 |
| 임신과 그에 관련된 병 pregnancy and related diseases | 18,086 |
| 감정 질환 emotional illness | 29.074 |
| 천식 asthma | 16,251 |
| 골격 질환 skeletal disease | 4,319 |
| 충수염 appendicitis | 7,801 |
| 폐렴 pneumonia | 5,679 |
| 담도질환 biliary tract disease | 5,663 |
| 전신질환 systemic disease | 7,455 |
| 피부와 피하조직 감염 skin and subcutaneous tissue infections | 5,914 |
| 정신 분열증 schizophrenia | 4,808 |
Sources and references: Trasande L Health Aff. 2009: 28: 751-760
Childhood obesity and treatment of obesity
• Because the causes of obesity are not simple and complex, treatment is difficult and complex.
- It is important to treat obesity in preschool children (Source: Pediatrics 8/2019)
• It is difficult to know exactly how many calories and nutrients they need every day to sustain basic human life, and how much physical and mental exercise they do every day.
• Because of this, it is difficult to treat obesity by controlling the amount of nutrients and calories from the daily food intake and the total energy (calories) and nutrients consumed in daily life.
• Children also need to eat a well-balanced diet for their age to keep growing and developing, while at the same time growing in weight and height every day.
• Also, the rate of weight gain varies from child to child. For these various complex reasons, childhood obesity is difficult to treat childhood obesity based on the uniform amount of food intake and physical exercise set based on the evidence.
• For this reason, it can be said that it is an ideal treatment for obesity in children to prevent obesity before it becomes obese.
• Take your child to the Pediatrics Department for regular pediatric health check-ups, measure their weight and height, find out what their weight mass index is, find out if they are obese, start treatment if they are obese, and prevent them from becoming obese.
• Obese children must eat three meals a day, just like non-obese children, with snacks and vitamins as needed.
• However, you should eat as few high-calorie foods as possible, such as cakes that contain more calories.
• There is a way to treat obesity by calculating the amount of calories that obese children need each day according to their age and weight and eating the corresponding food, but this method usually does not work well. • Severe obesity should be actively treated with pediatricians, pediatric psychiatrists, pediatric nutritionists, and parents and children as members of the obesity treatment team.
• Depending on the child’s weight, age, and daily physical activity level, the amount of calories needed for a day is calculated and the appropriate balanced diet is used, and psychotherapy and moderate physical exercise are sometimes used.
• In general, childhood obesity is not treated with drugs.
• Other types of obesity are treated with surgery.
• Studies show that eating a low-carb diet is more effective in controlling weight than eating a low-fat diet. Source: AMA Morning Rounds Wednesday, June 27, 2012
• Lorcaserin for the treatment of adult obesity has recently been approved by the US FDA. Lorcaserin can treat adult obesity with a BMI of 30 or more, type 2 diabetes, dyslipidemia or hypertension, and adult obesity with a BMI of 27 or more with appropriate physical exercise and food intake control.
• Not yet approved for use in the treatment of obesity in children under the age of 18. Physician’s First Watch for June 28, 2012
Obesity long-term treatment (adult)
비만 장기 치료제(성인)
|
Orlistat (Xenical) |
췌장 리파제 억제제로서 장관 지방 흡수 억제로 체중 감소 As a pancreatic lipase inhibitor, weight loss by inhibiting intestinal fat absorption |
|
Lorcaserin (Belviq) |
세로토닌 2C 수용체 작용제로 장기 비만 체중 감소 치료 Treatment of long-term obesity and weight loss with serotonin 2C receptor agonists |
|
Sibutramine (Reductil or Meridia) |
식욕 억제제 또는 식욕 부진제 Appetite suppressants or anorectics |
|
Rimonabant (Acomplia) |
식욕 부진제 anorexia pills |
|
Phentermine/topiramate |
약리 작용 잘 모름 the pharmacological action not known |
|
buproprion-naltraxone |
항 우울증 약 antidepressant drugs |
|
Liraglutide(Victoza) |
글루카곤 비슷 펲타이드 (GLP) 1 수용체 자용제로서 뇌 식욕 조절 Glucagon-like peptide (GLP) 1 receptor agonist to regulate brain appetite |
Source and reference: HARVARD MEDICAL SCHOOL, Endocrine CONTROVERSIES IN ADULT PRIMARY CARE PRACTICE MAY15~16 2015
Nelson Pediatrics Textbook 19th Ed
Table 5-2. The daily requirement of vitamins, proteins, minerals (minerals) and calories according to age, height, and weight
표 5-2.나이, 신장, 체중에 따른 비타민, 단백질, 미네랄(무기질), 칼로리의 1일 필요량
|
|
age (year) |
weight(kg) |
height(cm) |
calorie(kcal) |
protein(gm) |
calcium(gm) |
iron(mg) |
vitaminA I.U |
thiamin B1 (mg) |
riboflavin B2 (mg) |
niacin B3 (mg) |
vitamin C (mg)
|
vitamin D (mg) |
|
남여 영유아male and female infants |
0~1/2 |
7 |
63 |
115/kg |
2.0/kg |
0.6 |
1.0/kg |
1,500 |
0.4 |
0.4 |
6 |
35 |
400 |
|
1/2~1 |
9 |
72 |
100/kg |
1.8/kg |
0.6 |
15 |
1,500 |
0.5 |
0.6 |
8 |
35 |
400 |
|
|
male and female1~9years |
1~3 |
13 |
87 |
1,200/1 일 |
25/1 일 |
0.8 |
15 |
2,00 |
0.6 |
0.8 |
8 |
40 |
400 |
|
3~6 |
18 |
107 |
1,500/1 일 |
30/1 일 |
0.8 |
10 |
2,500 |
0.8 |
0.8 |
11 |
40 |
400 |
|
|
6~9 |
26 |
126 |
2,100/1 일 |
40/1 일 |
1.0 |
10 |
3,500 |
1.1 |
1.3 |
15 |
40 |
400 |
|
|
9~18 years male |
9~12 |
35 |
140 |
2,400/1 일 |
45/1 일 |
1.1 |
100 |
4,500 |
1.3 |
1.4 |
16 |
40 |
400 |
|
12~14 |
43 |
151 |
2,700/1 일 |
50/1 일 |
1.4 |
18 |
5,000 |
1.4 |
1.4 |
18 |
45 |
400 |
|
|
14~18 |
59 |
170 |
3,000/1 일 |
60/1 일 |
1.4 |
18 |
5.000 |
1.5 |
1.5 |
20 |
55 |
400 |
|
|
9~18 years female |
9~12 |
35 |
140 |
2,200/1 일 |
50/1 일 |
1.1 |
18 |
4,5000 |
1.1 |
1.3 |
15 |
40 |
400 |
|
12~14 |
44 |
154 |
2,300/1 일 |
50/1 일 |
1.3 |
18 |
5,000 |
1.2 |
1.5 |
15 |
45 |
400 |
|
|
14~18 |
53 |
158 |
2,300/1 일 |
55/1 일 |
1.3 |
18 |
5,000 |
1.2 |
1.5 |
15 |
50 |
400 |
| 나이 (년) |
weight (kg) |
height (cm) |
calorie (kcal) |
protein (g) |
calcium (g) |
iron (mg) |
vitamin A I.U. |
thiamin B1 (mg) |
riboplaminB2 (mg) |
niacin B3 (mg) |
vitamin C (mg) |
vitamin D (I.U.) |
|
| infant | 0~1/2 1/2~1 |
7 9 |
63 72 |
kgx115 kgx100 |
kgx2.0 1.8 |
0.5 0.6 |
kgx1.0 15 |
1,500 1,500 |
0.4 0.5 |
0.4 0.6 |
6 8 |
35 35 |
400 400 |
| 1~9 year s old male and female | 1~3 3~6 6~9 |
13 18 26 |
87 107 126 |
1,200 1,500 2,100 |
25 30 40 |
0.8 0.8 1.0 |
15 10 10 |
2,000 2,500 3,500 |
0.6 0.8 1.1 |
0.8 0.8 1.3 |
8 11 15 |
40 40 40 |
400 400 400 |
| 9~18 years old male and female | 9~12 12~14 14~18 |
35 43 59 |
140 151 170 |
2,400 2,700 3,000 |
45 50 60 |
1.1 1.4 1.4 |
10 18 18 |
4,500 5,000 5,000 |
1.3 1.4 1.5 |
1.4 1.4 1.5 |
16 18 20 |
40 45 55 |
400 400 400 |
| 9~18 years old female | 9~12 12~14 14~18 |
35 44 53 |
140 154 158 |
2,200 2,300 2,300 |
50 50 55 |
1.1 1.3 1.3 |
18 18 18 |
4,500 5,000 5,000 |
1.1 1.2 1.2 |
1.3 1.5 1.5 |
15 15 15 |
40 45 50 |
400 400 400 |
Surgical treatment of childhood obesity
• Severe obesity may cause co-morbidities (see p.113) such as hypertension, gastroesophageal reflux, apnea, bronchial asthma, degenerative joint disease, diabetes, and multiple ovarian cysts.
• When girls become obese and gain weight, puberty and puberty may occur earlier.
• Even 9-year-old girls can get puberty.
• Children who come to Puberty at this age may be able to produce children.
• Children who are severely obese and have co-morbidities such as hypertension, gastroesophageal reflux, apnea, bronchial asthma, degenerative joint disease, diabetes, or multiple ovarian cysts are actively treated with dietary obesity treatment, exercise obesity treatment, psycho-emotional obesity treatment, etc. If obesity is not properly treated even with treatment, it can be treated with surgical treatment of the Roux-en-Y gastric bypass after psychological evaluation and growth and development evaluation.
• However, complications such as pulmonary thrombosis, surgical site infection, gastric stenosis, gastric peptic ulcer, or small intestine obstruction may occur during treatment with bariatric surgery. • It is said that bariatric surgery can cure obesity in adolescents aged 12 to 19 years. • Laparoscopic gastric banding is sometimes used to treat obesity in American adolescent children (see Figure 1-84).
• Obesity in children who underwent surgery is said to be treated with sustained weight loss. Complications from surgery are said to be similar to those that occur during surgical treatment for obesity in adults.
Figure 1-84. Obesity Lasik Y type bypass surgery a – esophagus, b – newly created stoma sac, c – gastrojejunal anastomosis, d – adjustable stomach band, e – bypassed stomach, f – pylorus, g – jejunum, h – duodenum, i – stomach Source – Copyright ⓒ 2011 John Sangwon Lee, MD., FAAP
Children are obese
• If you have a BMI of 95 percent or higher and you have only one of the following, we recommend that you seek the advice of an appropriate specialist.
• o Diabetes – fasting blood sugar of 126 mg/dl or higher to 200 mg/dl o Impaired fasting blood sugar of 125-120 mg/dl
o 140-199 mg/dl in impaired fasting blood glucose compatibility test o The fasting blood sugar level is 25 or less
o Fasting LDL 160 or higher
o HDL below 40
o More than 300 triglycerides
o If polycystic ovary syndrome is suspected or
o If non-alcoholic fatty liver is suspected or
• If your BMI is at or above the 95th percentile and you have two or more of the following,
we recommend that you seek the advice of an appropriate specialist.
• o A sibling or fourth-degree sibling with type 2 diabetes, high blood pressure, early coronary artery disease, a stroke before age 55 for men, or stroke before age 65 for women;
o Micronigricans o Asian, Black, Hispanic, etc. Source: Connecticut Children’s Medical Center
The following is an example of Internet Child and Adolescent Health Counseling Questions and Answers on “Childhood Obesity”.
Q&A, childhood obesity Hello? I am a mother of a daughter who is now 5 years old. She has a habit of eating well and sleeping well since she was a baby, so she has been growing well without any ailments. What I want to ask the teacher is about the weight and height of children by age. Our daughter is now 5 years old, her birthday in March. She is 105 cm tall and weighs 19 kg. She is tall and a little chubby compared to the other kids, so she cares a lot. She says she controls her food at home, is there any concern she’s overweight? She’s a little worried.
A. Hello. Thanks for asking a good question. The more detailed information such as the child’s age, gender, past medical history, family history, examination findings, and clinical examination, the better we can give you an answer, but we will give you an answer based on the information you have given us.
Her weight is 75 percentile and her height is 10 percent. She’s a little bit fat. Both parents are probably a little overweight, just like their children. Please refer to obesity and if the problem still persists or if you are concerned, please consult a pediatrician and consult about the problem. If you have any more questions, please feel free to contact us again. thank you. Lee Sang-won Dream
출처 및 참조 문헌 Sources and references
- NelsonTextbook of Pediatrics 22ND Ed
- The Harriet Lane Handbook 22ND Ed
- Growth and development of the children
- Red Book 32nd Ed 2021-2024
- Neonatal Resuscitation, American Academy Pediatrics
- http://bit.obesitypre, 3/2015, Pediatrics
- 비만과 비만증에 관한 더 자세한 정보:
- Adolescent Health Update Vol. 21, No. 1 October 2008
- Obesity in Adolescence: Part 1
- Obesity in Adolescence: Part 2
- www.aap.org/obesity/American Academy of Pediatrics Overweight and Obesity Web site
- www.cdc.gov/nccdphp/dnpa/obesity
- www.mayoclinic.com/invoke.cfm?id=FL00058
- www.nal.usda.gov/fnic/etext/000060.html
- www.myoverweightchild.com
- www.healthinschools.org/sh/obesity.asp
- www.aps.nccd.cdc.gov/dnpabm/caculator.asp
- Connecticut Children’s Medical Center News Summer 2005소아가정간호백과–부모도 반의사가 되어야 한다, 이상원
- www.drleepediatrics.com 제1권 소아청소년 응급 의료
- www.drleepediatrics.com 제2권 소아청소년 예방
- www.drleepediatrics.com 제3권 소아청소년 성장 발육 육아
- www.drleepediatrics.com 제4권 모유,모유수유, 이유
- www.drleepediatrics.com 제5권 인공영양, 우유, 이유식, 비타민, 미네랄, 단백질, 탄수화물, 지방
- www.drleepediatrics.com 제6권 신생아 성장 발육 육아 질병
- www.drleepediatrics.com제7권 소아청소년 감염병
- www.drleepediatrics.com제8권 소아청소년 호흡기 질환
- www.drleepediatrics.com제9권 소아청소년 소화기 질환
- www.drleepediatrics.com제10권. 소아청소년 신장 비뇨 생식기 질환
- www.drleepediatrics.com제11권. 소아청소년 심장 혈관계 질환
- www.drleepediatrics.com제12권. 소아청소년 신경 정신 질환, 행동 수면 문제
- www.drleepediatrics.com제13권. 소아청소년 혈액, 림프, 종양 질환
- www.drleepediatrics.com제14권. 소아청소년 내분비, 유전, 염색체, 대사, 희귀병
- www.drleepediatrics.com제15권. 소아청소년 알레르기, 자가 면역질환
- www.drleepediatrics.com제16권. 소아청소년 정형외과 질환
- www.drleepediatrics.com제17권. 소아청소년 피부 질환
- www.drleepediatrics.com제18권. 소아청소년 이비인후(귀 코 인두 후두) 질환
- www.drleepediatrics.com제19권. 소아청소년 안과 (눈)질환
- www.drleepediatrics.com 제20권 소아청소년 이 (치아)질환
- www.drleepediatrics.com 제21권 소아청소년 가정 학교 간호
- www.drleepediatrics.com 제22권 아들 딸 이렇게 사랑해 키우세요
- www.drleepediatrics.com 제23권 사춘기 아이들의 성장 발육 질병
- www.drleepediatrics.com 제24권 소아청소년 성교육
- www.drleepediatrics.com 제25권 임신, 분만, 출산, 신생아 돌보기
- Red book 29th-31st edition 2021
- Nelson Text Book of Pediatrics 19th- 21st Edition
- The Johns Hopkins Hospital, The Harriet Lane Handbook, 22nd edition
- 응급환자관리 정담미디어
- Pediatric Nutritional Handbook American Academy of Pediatrics
- 소아가정간호백과–부모도 반의사가 되어야 한다, 이상원 저
- The pregnancy Bible. By Joan stone, MD. Keith Eddleman, MD
- Neonatology Jeffrey J. Pomerance, C. Joan Richardson
- Preparation for Birth. Beverly Savage and Dianna Smith
- 임신에서 신생아 돌보기까지. 이상원
- Breastfeeding. by Ruth Lawrence and Robert Lawrence
- Sources and references on Growth, Development, Cares, and Diseases of Newborn Infants
- Emergency Medical Service for Children, By Ross Lab. May 1989. p.10
- Emergency care, Harvey Grant and Robert Murray
- Emergency Care Transportation of Sick and Injured American Academy of Orthopaedic Surgeons
- Emergency Pediatrics A Guide to Ambulatory Care, Roger M. Barkin, Peter Rosen
- Quick Reference To Pediatric Emergencies, Delmer J. Pascoe, M.D., Moses Grossman, M.D. with 26 contributors
- Neonatal resuscitation Ameican academy of pediatrics
- Pediatric Nutritional Handbook American Academy of Pediatrics
- Pediatric Resuscitation Pediatric Clinics of North America, Stephen M. Schexnayder, M.D.
-
Pediatric Critical Care, Pediatric Clinics of North America, James P. Orlowski, M.D.
-
Preparation for Birth. Beverly Savage and Dianna Smith
-
Infectious disease of children, Saul Krugman, Samuel L Katz, Ann A.
- 제4권 모유, 모유수유, 이유 참조문헌 및 출처
- 제5권 인공영양, 우유, 이유, 비타민, 단백질, 지방 탄수 화물 참조문헌 및 출처
- 제6권 신생아 성장발육 양호 질병 참조문헌 및 출처
- 소아과학 대한교과서
Copyright ⓒ 2014 John Sangwon Lee, MD., FAAP
“부모도 반의사가 되어야 한다”-내용은 여러분들의 의사로부터 얻은 정보와 진료를 대신할 수 없습니다.
“The information contained in this publication should not be used as a substitute for the medical care and advice of your doctor. There may be variations in treatment that your doctor may recommend based on individual facts and circumstances.
“Parental education is the best medicine.